I guess the point is that it shows the correlation between processed food and cancer is statistically significant. As in there is definitely a link, and this meta analysis shows good evidence this link exists. Even if the impact is small.
As for the day to day impact of this study, I’m not sure there is one. Processed food is already on WHOs list of things that definitely cause cancer.
Getting a colorectal cancer probability in a lifetime is about 0.04, eating hotdog adds 8% to it or ~0.003.
Depending on the average amount of processed meats eaten, it could also show not eating a hot dog every day will reduce your risk of cancer by about that much. It’s probably only important in the cumulative though. When we have studies like this for many foods, you could put together a diet that reduces your chance of cancer by 20 or 30%, say. But one food’s impact like this is probably only important to scientists.
1000 people show up to the annual picnic. If we remove hot dogs from the market, and dont serve them at our picnic, or any picnic, ever, 40 of those 1000 people are going to get colorectal cancer.
If we do serve hot dogs at our picnic (and every other picnic), 43 people are going to get colorectal cancer at some point in their lives.
It’s probably only important in the cumulative though. When we have studies like this for many foods, you could put together a diet that reduces your chance of cancer by 20 or 30%, say.
I don’t think that quite transfers, epidemiology is very weak, it only surfaces associates which is a good point to do a interventional trial but that is rarely done. The core problem with these studies is that to isolate variables they have to make a model of that variable in isolation, this relies on both assumptions of the model maker, accuracy of data, and is very vulnerable to p-hacking. Model assumptions that a hamburger and fries counts as meat, but not vegetable (potato) also impact the outcomes.
The large observational food surveys conducted typically have a 1-4 year questionnaire about how many servings of different food someone ate. Once every 4 years leaves lots of room open for forgetfulness.
There is a huge problem with healthy user confounders, people trying to follow all the modern health advice are going to skew results - not because all of the advice is correct, but some of it is. If someone exercises regularly, practices mindfulness, avoids processed foods, avoids meat - Are their improvements due to any single variable, yet on a food survey they get over represented because of these exclusionary behaviors.
We also have multiple different epidemiology studies covering the same topics and getting different results, that probably means we are focusing on the wrong question, it’s noisy.
From my reading its far more likely the modern epidemic of chronic disease is caused by the introduction of excessive carbohydrates in processed foods, the novel addition of industrial oils (again processed foods) into the food supply - they account for 30%!!! of the average westerners average calorie intake, exposure to food contaminates from agrochemicals such as pesticides. The metabolic context of people filling out these surveys is a critical part that is being omitted.
In the following graphs notice how the incidence is very high in countries with traditionally low meat consumption like india? This indicates the hypothesis generated from the abstract paper isn’t asking the right question.
example graphs
CVD
Type 2 Diabetes
My point is that you can follow every bit of advice from associative food surveys, but since the wrong questions are being focused on, your outcomes wont be as good as you hope. Quite frankly epidemiology is more about publicity and marketing then being part of the scientific process.
If you haven’t read about the Metabolic Theory of Cancer I highly recommend giving it a read. It’s a much more compelling model, and explains the surge of cancer since 1900, as well as actionable steps to reduce incidence (reduce sugar and inflammation).
Like I said, it may be a scientifically interesting study, but the broader audience can’t take anything from it but anxiety.
a diet that reduces your chance of cancer by 20 or 30%, say.
That would be significant, but probably not today. The lifetime risk of dying as a pedestrian in a car accident is around 1 in 100, so mitigating other risks is not an option for now
Cancer is the leading cause of premature mortality and morbidity (death and disability) in Canada.
So, an accumulation of small risks, and avoidance of risks, have significant benefits at both the individual and population levels.
The general population needs to be aware that unhealthy eating is impacting their lives and quality of life.
Let’s stick to the peer reviewed science and evidence consensus.
WHO established the four behavioural common risk factors for the four major chronic noncommunicable diseases decades ago.
The kind of research synthesis in this article is about continuing to build the evidence on relative and absolute risks, and in some cases look at how these differences impact different populations more or less due to intersecting determinants.
My point is that raising risks of getting hit by a car, or other accidental causes of injury and death beyond the individual’s control, is a deflection.
Cancer is the leading cause of death in Canada.
Full stop.
No one single risk factor is responsible for that. Building the evidence base to be able to both inform individual behaviour but also to inform food safety regulations is important.

I guess the point is that it shows the correlation between processed food and cancer is statistically significant. As in there is definitely a link, and this meta analysis shows good evidence this link exists. Even if the impact is small.
As for the day to day impact of this study, I’m not sure there is one. Processed food is already on WHOs list of things that definitely cause cancer.
Depending on the average amount of processed meats eaten, it could also show not eating a hot dog every day will reduce your risk of cancer by about that much. It’s probably only important in the cumulative though. When we have studies like this for many foods, you could put together a diet that reduces your chance of cancer by 20 or 30%, say. But one food’s impact like this is probably only important to scientists.
So getting back to your original question:
Yes. Anxiety drives clicks which drives revenue.
1000 people show up to the annual picnic. If we remove hot dogs from the market, and dont serve them at our picnic, or any picnic, ever, 40 of those 1000 people are going to get colorectal cancer.
If we do serve hot dogs at our picnic (and every other picnic), 43 people are going to get colorectal cancer at some point in their lives.
Pass the mustard.
I don’t think that quite transfers, epidemiology is very weak, it only surfaces associates which is a good point to do a interventional trial but that is rarely done. The core problem with these studies is that to isolate variables they have to make a model of that variable in isolation, this relies on both assumptions of the model maker, accuracy of data, and is very vulnerable to p-hacking. Model assumptions that a hamburger and fries counts as meat, but not vegetable (potato) also impact the outcomes.
The large observational food surveys conducted typically have a 1-4 year questionnaire about how many servings of different food someone ate. Once every 4 years leaves lots of room open for forgetfulness.
There is a huge problem with healthy user confounders, people trying to follow all the modern health advice are going to skew results - not because all of the advice is correct, but some of it is. If someone exercises regularly, practices mindfulness, avoids processed foods, avoids meat - Are their improvements due to any single variable, yet on a food survey they get over represented because of these exclusionary behaviors.
We also have multiple different epidemiology studies covering the same topics and getting different results, that probably means we are focusing on the wrong question, it’s noisy.
From my reading its far more likely the modern epidemic of chronic disease is caused by the introduction of excessive carbohydrates in processed foods, the novel addition of industrial oils (again processed foods) into the food supply - they account for 30%!!! of the average westerners average calorie intake, exposure to food contaminates from agrochemicals such as pesticides. The metabolic context of people filling out these surveys is a critical part that is being omitted.
In the following graphs notice how the incidence is very high in countries with traditionally low meat consumption like india? This indicates the hypothesis generated from the abstract paper isn’t asking the right question.
example graphs
CVD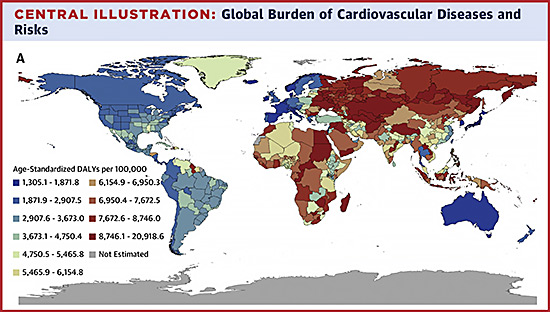
Type 2 Diabetes
My point is that you can follow every bit of advice from associative food surveys, but since the wrong questions are being focused on, your outcomes wont be as good as you hope. Quite frankly epidemiology is more about publicity and marketing then being part of the scientific process.
If you haven’t read about the Metabolic Theory of Cancer I highly recommend giving it a read. It’s a much more compelling model, and explains the surge of cancer since 1900, as well as actionable steps to reduce incidence (reduce sugar and inflammation).
Like I said, it may be a scientifically interesting study, but the broader audience can’t take anything from it but anxiety.
That would be significant, but probably not today. The lifetime risk of dying as a pedestrian in a car accident is around 1 in 100, so mitigating other risks is not an option for now
Cancer is the leading cause of premature mortality and morbidity (death and disability) in Canada.
So, an accumulation of small risks, and avoidance of risks, have significant benefits at both the individual and population levels.
The general population needs to be aware that unhealthy eating is impacting their lives and quality of life.
Let’s stick to the peer reviewed science and evidence consensus.
WHO established the four behavioural common risk factors for the four major chronic noncommunicable diseases decades ago.
The kind of research synthesis in this article is about continuing to build the evidence on relative and absolute risks, and in some cases look at how these differences impact different populations more or less due to intersecting determinants.
Common risk factors
Major chronic noncommunicable diseases
No questions regarding the populational risks as the small percentages would shine with the big numbers.
WHO’s recommendations remain the same for decades indeed: lower processed and red meat, eat chicken and fiber.
What’s your point exactly?
My point is that raising risks of getting hit by a car, or other accidental causes of injury and death beyond the individual’s control, is a deflection.
Cancer is the leading cause of death in Canada.
Full stop.
No one single risk factor is responsible for that. Building the evidence base to be able to both inform individual behaviour but also to inform food safety regulations is important.